


How Long Does It Take for a 1,000 mL IV Drip Saline Bag to Empty?
The 1,000 mL IV bag is the standard workhorse of inpatient infusion therapy. Whether it is normal saline, lactated Ringer’s, or another isotonic crystalloid, the time it takes to infuse depends directly on the ordered flow rate.
At the most common maintenance rate of 100 mL/hr, a 1,000 mL bag runs for exactly 10 hours. At 83 mL/hr, a rate equivalent to 2 liters per day, it takes approximately 12 hours. Understanding these intervals helps nursing staff plan bag changes, coordinate medication timing, and verify that programmed rates match clinical orders.
What Is the Formula for Calculating IV Infusion Time?
The formula is the same regardless of bag volume:
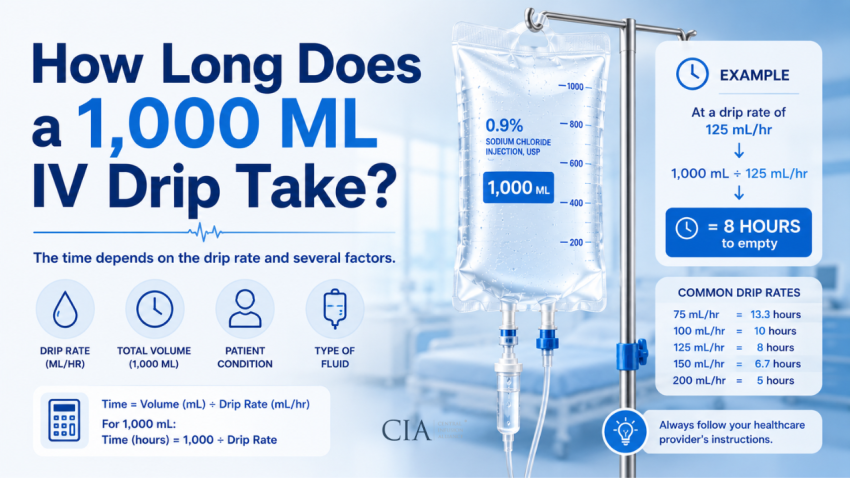
Infusion Time (hours) = Volume (mL) / Flow Rate (mL/hr)
For a 1,000 mL bag: Time = 1,000 / Flow Rate.
Convert decimal hours to minutes by multiplying the decimal portion by 60. For example, 1,000 / 75 = 13.33 hours = 13 hours and 20 minutes (0.33 x 60 = 20 minutes).
This calculation gives the theoretical infusion time assuming uninterrupted flow. In practice, pump pauses, alarm responses, line manipulations, and patient repositioning add time to the actual duration.
How Long Does a 1,000 mL Bag Take at Common Flow Rates?
The table below covers the range of flow rates used in clinical practice, from fluid-restricted maintenance through active resuscitation:
| Flow Rate (mL/hr) | Infusion Time | Clinical Context |
| 50 mL/hr | 20 hours | Fluid-restricted patients (CHF, CKD, cirrhosis) |
| 75 mL/hr | ~13.3 hours | Conservative maintenance, overnight infusion |
| 83 mL/hr | ~12 hours | Standard maintenance (approximately 2 L/day) |
| 100 mL/hr | 10 hours | Standard adult maintenance hydration |
| 125 mL/hr | 8 hours | Rehydration or maintenance for most adults |
| 150 mL/hr | ~6.7 hours | Active rehydration, moderate fluid deficits |
| 200 mL/hr | 5 hours | Rapid infusion, pre-procedure loading |
| 250 mL/hr | 4 hours | Resuscitation phase, bolus administration |
How Do You Calculate Drip Rate for a 1,000 mL Bag Without a Pump?
When an infusion pump is not available, gravity administration requires calculating the drip rate in drops per minute. The formula is:
gtt/min = (Volume in mL x Drop Factor) / Time in minutes
Drop factor is determined by the IV administration set used. Macrodrip sets are available in 10 gtt/mL or 15 gtt/mL; microdrip sets deliver 60 gtt/mL. The drop factor is printed on the set packaging and must be confirmed before calculation.
Worked Examples at 100 mL/hr (Standard Rate)
10 gtt/mL set: 1,000 x 10 / 600 minutes = 16.7, rounded to 17 gtt/min.
15 gtt/mL set: 1,000 x 15 / 600 minutes = 25 gtt/min exactly.
60 gtt/mL set: 1,000 x 60 / 600 minutes = 100 gtt/min. At this rate, a microdrip set is not practical; use a macrodrip set or pump.
Worked Examples at 125 mL/hr (8-Hour Bag)
10 gtt/mL set: 1,000 x 10 / 480 minutes = 20.8, rounded to 21 gtt/min.
15 gtt/mL set: 1,000 x 15 / 480 minutes = 31.25, rounded to 31 gtt/min.
When using a 60 gtt/mL microdrip set with a 1,000 mL bag at low flow rates (under 60 mL/hr), the shortcut still holds: gtt/min equals mL/hr numerically.
Why Is the 1,000 mL Bag the Most Commonly Used IV Bag Size?
The 1,000 mL bag became the clinical standard for several practical reasons. At typical adult maintenance rates of 75 to 125 mL/hr, a single 1,000 mL bag covers 8 to 13 hours, roughly one nursing shift or an overnight period. This minimizes the frequency of bag changes, reducing nursing workload and line manipulation events (each manipulation being a potential source of contamination).
From a supply and procurement standpoint, the 1,000 mL size offers the lowest cost per mL compared to smaller bag sizes. Pharmacy preparation of piggyback medications also defaults to the 1,000 mL bag as a primary diluent when large volumes are needed for admixtures.
The bag is compatible with standard IV sets, blood/medication filters, and most pump systems without requiring adapter modifications. For patients without fluid restrictions, the 1,000 mL bag requires no clinical trade-offs.
What Factors Affect How Long a 1,000 mL Bag Will Actually Take?
Several variables can extend or shorten the calculated infusion time:
- Pump accuracy: Volumetric pumps typically operate within +/- 5% accuracy under normal conditions. At 100 mL/hr, this means actual delivery may be 95 to 105 mL/hr, shifting a 10-hour calculated time by up to 30 minutes in either direction.
- Occlusion events: Partial line occlusions from kinked tubing, positional occlusions, or fibrin sheaths on catheter tips slow flow without triggering immediate pump alarms on all pump models.
- Air elimination: Most pumps with inline air detectors pause when microbubbles are detected. Repeated pauses add meaningful time to long infusions.
- Piggyback competition: When secondary (piggyback) medications are infusing, the primary line typically stops. Total 1,000 mL bag infusion time extends by the cumulative piggyback infusion time.
- Gravity infusion variables: For gravity drips, bag height, tubing length, filter resistance, and patient arm position all affect actual drip rate and must be rechecked every 1 to 2 hours.
- Rate changes: If the clinical team adjusts the rate during infusion, remaining time must be recalculated. Many nurses and techs fail to do this, leading to discrepancies between the original schedule and actual completion.
What Happens If a 1,000 mL IV Bag Runs Dry?
A bag running completely dry creates several problems. Air enters the drip chamber and tubing, triggering air-in-line alarms on most infusion pumps. The pump stops. Clearing the air requires purging the line, which adds nursing time and creates an additional touch point on the IV circuit.
For most crystalloid infusions, a brief dry period is a nuisance, not a clinical emergency. However, for critically important continuous infusions, vasopressors, concentrated electrolytes, insulin drips, heparin, sedation, even a 5- to 10-minute interruption can produce clinically significant effects.
Prevention is straightforward: proactive monitoring. Assess IV bag volume at every nursing check. Prepare and prime the next bag when the current bag has approximately 50 to 100 mL remaining. For high-risk infusions, set an infusion pump end-of-infusion reminder 15 to 30 minutes before calculated completion.
Some facilities use volume-based alerts on their smart pump systems, which alarm at a configurable remaining-volume threshold rather than waiting for empty detection. This is the preferred approach for uninterrupted critical infusions.
References
- https://pubmed.ncbi.nlm.nih.gov/37492690/
- https://www.ncbi.nlm.nih.gov/books/NBK593207/
- https://www.ncbi.nlm.nih.gov/books/NBK596734/
- https://www.ncbi.nlm.nih.gov/books/NBK545210/
- https://www.ncbi.nlm.nih.gov/books/NBK532305/
- https://www.ncbi.nlm.nih.gov/books/NBK554180/
- https://www.fda.gov/medical-devices/infusion-pumps/examples-reported-infusion-pump-problems
- https://www.cdc.gov/infection-control/hcp/intravascular-catheter-related-infection/prevention-strategies.html
- https://www.bd.com/content/dam/bd-assets/na/medication-management-solutions/documents/brochure/IF_Alaris-Pump-Module_FQ_EN.pdf

