


IV Cannula Gauge Sizes, Colors, Flow Rates, and Usage (with Chart)
Selecting the correct IV cannula gauge is a foundational clinical decision. The wrong choice can mean inadequate flow during resuscitation, unnecessary phlebitis in a patient who only needed routine hydration, or failed contrast injection for a time-sensitive CT scan.
Every gauge in the standard range has a specific role determined by its inner diameter, resulting flow rate, and the vein it fits. This article covers the full gauge spectrum from 14G to 26G with the ISO color code, diameter, flow rate, and the clinical scenarios where each is appropriate.
How Does IV Cannula Gauge Sizing Work?
IV cannula gauges follow the Birmingham Wire Gauge (BWG) system, which is an inverse measurement: the higher the gauge number, the smaller the outer diameter. A 14G cannula has a much larger lumen than a 22G. This inverse relationship confuses newer clinicians but is consistent across all needle and cannula gauge systems.
Flow rate through a catheter is governed by Poiseuille’s Law: flow is proportional to the fourth power of the radius. This means small changes in diameter produce large changes in flow. Doubling the radius increases flow by a factor of 16. In practical terms: the difference between a 16G and a 20G is not incremental. A 16G delivers approximately 180 mL/min; a 20G delivers approximately 60 mL/min. That 3-fold difference is life-altering in acute hemorrhage.
IV Cannula Gauge Size Chart
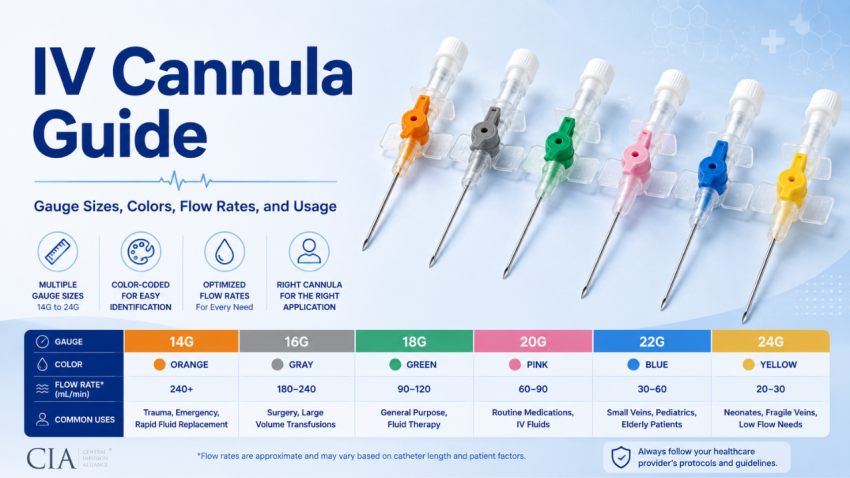
The table below lists the full range of peripheral IV cannula gauges in common clinical use, with ISO 10555-5 color coding, physical dimensions, approximate flow rates, and primary indications:
| Gauge | ISO Color | Outer Diameter | Approx. Flow Rate | Primary Uses |
| 14G | Orange | 2.0 mm | ~270 mL/min | Major trauma, rapid volume resuscitation, large-volume OR cases |
| 16G | Grey | 1.7 mm | ~180 mL/min | Surgery, blood transfusion, rapid large-volume infusion |
| 17G | White | 1.4 mm | ~125 mL/min | Blood transfusion, general use (less common gauge) |
| 18G | Green | 1.2 mm | ~90 mL/min | Blood products, CT contrast injection, general IV access |
| 20G | Pink | 1.0 mm | ~60 mL/min | Standard adult medications, hydration, most wards |
| 22G | Blue | 0.8 mm | ~36 mL/min | Pediatric patients, elderly, fragile veins |
| 24G | Yellow | 0.7 mm | ~22 mL/min | Neonates, oncology patients, very fragile veins |
| 26G | Violet | 0.6 mm | ~12 mL/min | Neonates, extremely small or fragile veins |
Note: Flow rates listed are approximate values under standardized gravity conditions and will vary with patient-specific factors including blood viscosity, venous pressure, infusion height, and tubing resistance. Values are consistent with published manufacturer data and the INS Infusion Therapy Standards of Practice (2021).
What IV Gauge Should You Use? (Clinical Decision Guide)
When to Use 14G to 16G (Large Bore)
These gauges are reserved for situations where maximum flow rate is the clinical priority.
- Trauma resuscitation: ATLS (Advanced Trauma Life Support) protocol specifies two large-bore IVs as the first step in hemorrhagic shock management. Minimum gauge recommended is 18G, but 16G or 14G is preferred. The 14G delivers approximately 270 mL/min, essential when infusing blood products or crystalloid at resuscitation volumes.
- Major surgery: Anesthesia teams insert 16G or 14G cannulas preoperatively for procedures with anticipated significant blood loss.
- Rapid volume resuscitation: Any scenario requiring infusion rates above 100 to 150 mL/min, massive transfusion protocol, septic shock with refractory hypotension, requires large bore access.
- Note: These large gauges are painful to insert and more likely to cause phlebitis. Do not use routinely when smaller gauges are clinically adequate.
When to Use 18G (Workhorse Size)
The 18G is the most versatile adult gauge. It flows fast enough for blood products and CT contrast injection (minimum 18G is required by most CT protocols for power injection) while being tolerable in most adult peripheral veins. Antecubital and forearm veins typically accommodate 18G without difficulty.
- Blood transfusion: 18G is the minimum recommended gauge for packed red blood cell transfusion to prevent hemolysis from excessive shear stress through the cannula lumen.
- CT contrast power injection: Radiology departments typically require 18G or larger for contrast power injection at rates of 2 to 5 mL/sec.
- General adult IV access when larger volumes or faster rates may be needed.
When to Use 20G to 22G (Standard to Small)
The 20G is the standard for most adult inpatient IV access when blood products and high-rate infusion are not anticipated. It accommodates the majority of IV medications, hydration, and intermittent infusions without difficulty.
- Routine IV medications: antibiotics, antiemetics, electrolyte replacement, PCA pumps
- Maintenance hydration
- 22G is appropriate for patients with difficult venous access where 20G cannot be placed reliably, thin-walled veins, multiple failed attempts, or elderly patients with fragile veins
- 22G is also appropriate for short-term access in children over approximately 3 years of age
When to Use 24G to 26G (Pediatric and Neonatal)
These fine-gauge cannulas are designed for neonates, premature infants, and patients with extremely small or fragile peripheral veins.
- Neonates and premature infants: scalp veins, dorsal foot, wrist, sites with minimal subcutaneous tissue that cannot accommodate larger gauges
- Oncology patients: after repeated chemotherapy cycles, peripheral veins become scarred and fragile; 24G or 26G may be the only viable peripheral option
- Flow rates at 24G to 26G are low (12 to 22 mL/min). Not suitable for rapid infusion or blood products without accepting prolonged infusion times.
How Does Gauge Size Affect Flow Rate?
The relationship between gauge and flow follows Poiseuille’s Law, where flow rate scales with the fourth power of the inner radius. In practical terms, each step change in gauge from 14G to 26G reduces the achievable flow rate substantially.
The clinical implication is that you cannot compensate for an inadequate gauge by increasing infusion pump rate. A pump set to deliver 500 mL/hr through a 22G cannula will alarm on occlusion before achieving that rate. Large-volume or high-rate infusions require large-bore access, the physics are not negotiable.
Viscous fluids amplify these differences. Packed red blood cells are significantly more viscous than saline. At equivalent driving pressure, blood flows more slowly through a given gauge than crystalloid. This is why 18G is the minimum for blood transfusion, below that gauge, transit time increases hemolysis risk and transfusion duration becomes impractical.
What Is the ISO Color Coding Standard for IV Cannulas?
ISO 10555-5 establishes a standardized color coding system for intravascular catheters. The color corresponds to the gauge and is consistent across manufacturers who comply with the standard. This allows clinicians to identify gauge size at a glance without reading packaging text, important in high-acuity situations.
The color-to-gauge mapping (Orange=14G, Grey=16G, White=17G, Green=18G, Pink=20G, Blue=22G, Yellow=24G, Violet=26G) is used by major manufacturers including BD (Becton Dickinson), B. Braun, Terumo, and Smiths Medical. However, compliance with ISO 10555-5 color coding is not universally mandated in all countries. When using non-standard suppliers, verify gauge on the packaging rather than relying solely on hub color.
What Complications Are Associated With IV Gauge Selection?
Gauge selection affects both insertion success and complication rates.
- Phlebitis: Larger gauges in small veins create mechanical irritation at the cannula tip and along the vessel wall. A 16G in a small hand vein will almost certainly cause chemical and mechanical phlebitis within 12 to 24 hours.
- Infiltration and extravasation: Larger cannulas in fragile veins are more likely to breach the vessel wall, particularly with repeated movement or in patients with thin tissue.
- Hemolysis: Using a gauge below 18G for blood transfusion increases shear stress on red blood cells passing through the lumen, potentially causing hemolysis and rendering the transfusion less effective.
- Insertion failure: Attempting a large gauge in a small or rolling vein increases failed insertion attempts, patient discomfort, and time to vascular access. Matching gauge to available venous anatomy is essential.
- Thrombosis: Repeated large-gauge insertions in the same vein segment cause endothelial damage and thrombotic occlusion.
How Does Vein Selection Relate to IV Gauge?
Vein selection and gauge selection are interdependent decisions. As a general rule, the cannula should occupy no more than one-third to one-half the diameter of the target vein. A cannula that nearly fills the vein impairs blood flow around it, concentrates irritants, and causes mechanical endothelial damage.
Large antecubital veins (median cubital, cephalic at the elbow) can accommodate 16G to 18G. Forearm veins, cephalic and basilic in the mid-forearm, typically accommodate 18G to 20G comfortably. Hand and wrist veins usually support 20G to 22G. Digital veins and scalp veins in neonates require 24G to 26G.
Avoid the antecubital fossa for routine access when possible, joint flexion occludes cannulas positioned at the bend. Reserve it for emergency large-bore access when no forearm veins are available.
References
- https://pubmed.ncbi.nlm.nih.gov/33394637/
- https://pubmed.ncbi.nlm.nih.gov/16356500/
- https://www.ncbi.nlm.nih.gov/books/NBK534830/
- https://www.ncbi.nlm.nih.gov/books/NBK499824/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC9832806/
- https://gravitas.acr.org/PPTS/GetDocumentView?docId=166
- https://journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0252166
- https://cdn.standards.iteh.ai/samples/54885/ada0fd5628fa4ad1a5cdc48d6811be42/ISO-10555-5-2013.pdf
- https://www.cdc.gov/infection-control/hcp/intravascular-catheter-related-infection/prevention-strategies.html

