


What Is Considered a Large Bore vs. Small Bore IV?
The terms large bore and small bore are used loosely in clinical practice but carry specific meaning when treatment decisions depend on them. In an emergency, active hemorrhage, anaphylaxis, hemodynamic collapse, bore size determines whether enough fluid or blood can be delivered fast enough to keep the patient alive. Getting this right is not a nuance. It is the difference between adequate and inadequate resuscitation.
What Is a Large Bore IV?
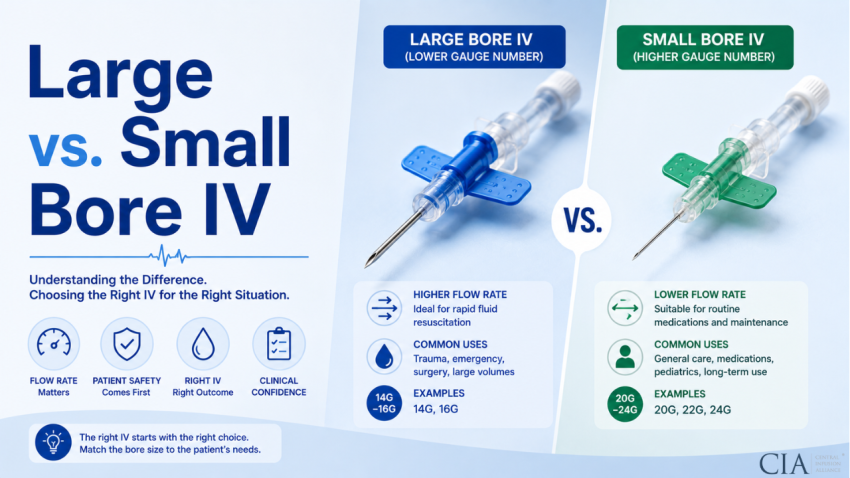
Large bore IV access is generally defined as a peripheral intravenous catheter with a gauge of 18 or larger, meaning 18G, 16G, or 14G. However, within that range, clinical definitions narrow further depending on context.
For trauma and hemorrhagic shock, the practical standard for large bore is 16G or 14G. At 16G, approximate maximum flow through a peripheral IV is around 180 mL/min under gravity with normal saline. At 14G, that climbs to approximately 270 mL/min. These are the rates that enable meaningful volume resuscitation in the timeframes required for hemorrhagic shock management.
The 18G is often included in the large bore category for purposes such as blood transfusion (minimum for packed red cells without excessive hemolysis) and CT contrast power injection (most radiology protocols require at least 18G). In everyday hospital use, 18G represents the lower threshold of what many clinicians call large bore.
What Is a Small Bore IV?
Small bore typically refers to gauges of 20G and smaller, meaning 20G, 22G, 24G, and 26G. These cannulas are appropriate for the majority of routine inpatient IV access.
A 20G delivers approximately 60 mL/min, which is more than adequate for most IV medications, maintenance hydration, and intermittent infusions. It is not adequate for rapid volume resuscitation. A 22G delivers around 36 mL/min, fine for antibiotics and moderate-rate infusions, but insufficient for blood products or contrast injection. At 24G and 26G, flow rates drop to 22 and 12 mL/min respectively; these are neonatal and fragile-vein gauges.
Why Does Bore Size Matter in Clinical Practice?
Flow rate through a catheter scales with the fourth power of the inner radius (Poiseuille’s Law). The practical consequence: a 16G cannula flows at roughly 3 times the rate of a 20G cannula. A 14G flows at more than 4 times the rate of a 20G.
In routine care, these differences are irrelevant. Most IV medications are infused over 30 to 60 minutes, and any gauge from 18G to 22G will accommodate them without difficulty.
In an emergency, those differences are everything. Consider a patient in Class III hemorrhagic shock who needs 2 liters of crystalloid and 2 units of packed red blood cells urgently. Through a single 20G at maximum gravity flow (around 60 mL/min), delivering 2 liters takes over 30 minutes under ideal conditions. Through a 16G, the same volume takes around 11 minutes. That 20-minute difference is clinically significant.
When Is a Large Bore IV Required?
Specific clinical situations demand large bore access as a standard of care:
- Trauma and hemorrhagic shock: ATLS protocol requires two large-bore (minimum 18G, preferred 16G or 14G) peripheral IVs as the first step in resuscitation. This is not a suggestion; it is the established standard for initial trauma management. Speed of vascular access and flow capacity directly impact survival in hemorrhagic shock.
- Massive transfusion protocol (MTP): Delivering blood products at the ratios and rates required in MTP (typically 1:1:1, packed red cells, fresh frozen plasma, platelets) requires large-bore access. 16G or larger is standard; many trauma centers insert an introducer sheath for maximum flow capacity.
- Rapid fluid resuscitation: Septic shock, anaphylaxis, and burns requiring aggressive initial fluid loading all benefit from large-bore access. The surviving sepsis campaign’s initial 30 mL/kg crystalloid bolus for septic shock is achievable through 18G in most patients but is best completed rapidly through 16G or larger.
- CT contrast power injection: Most radiology power injectors require minimum 18G placed in the antecubital fossa or a large forearm vein. Power injection rates of 3 to 5 mL/sec cannot be safely administered through smaller gauges due to extravasation risk under the pressure generated by the injector.
- Major surgery and anesthesia: Anesthesiologists routinely insert 16G or 14G for any procedure with anticipated blood loss. Intraoperative fluid and blood management requires the capacity to infuse rapidly when needed.
When Is a Small Bore IV Appropriate?
Small bore (20G to 22G) is appropriate for the majority of non-emergency clinical scenarios:
- Routine IV antibiotics, antiemetics, and other scheduled IV medications
- Maintenance IV hydration at rates of 75 to 125 mL/hr
- Patient-controlled analgesia (PCA) pump access
- Intermittent IV medication administration with flush-to-lock intervals
- Patients with limited venous access where larger gauges cannot be placed without undue risk
Using small bore when small bore is adequate conserves larger veins for future access, reduces insertion pain, and lowers the rate of mechanical phlebitis. The principle is to use the smallest gauge that meets the clinical requirement, not the largest available.
What Happens If You Use a Small Bore IV When a Large Bore Is Needed?
In a resuscitation scenario, a small bore IV creates a flow bottleneck that no pump setting can overcome. A pump set to deliver 500 mL/hr through a 22G will alarm on occlusion within seconds because the catheter physically cannot sustain that flow rate. Even if it does not alarm, delivery will be far below the ordered rate.
Blood products pushed rapidly through a sub-18G catheter generate significant shear stress in the lumen, increasing the risk of red cell hemolysis and rendering the transfusion less therapeutically effective. This is why 18G is the established minimum for blood transfusion.
Contrast extravasation during power injection through a small-bore cannula is a recognized complication. Contrast media injected under mechanical pressure through a compromised or undersized cannula can extravasate into the surrounding tissue, causing chemical tissue injury ranging from mild swelling to compartment syndrome.
What Are the Large Bore IV Alternatives When Peripheral Access Fails?
When large-bore peripheral access cannot be established, several alternatives exist:
- Intraosseous (IO) access: Placed in the humeral head, proximal tibia, or distal tibia using a powered drill or impact device (EZ-IO, BIG). Adult humeral head IO access can deliver fluids at rates comparable to a 16G peripheral IV when pressurized infusion is used. IO access can be established in under 60 seconds by a trained provider, making it the preferred emergency alternative when peripheral access fails after two attempts or 90 seconds.
- Introducer sheath (large-bore central access): An 8.5 French introducer sheath placed via the Seldinger technique in the femoral, subclavian, or internal jugular vein provides the highest peripheral-equivalent flow available through a single-lumen device. The inner diameter of an 8.5 Fr sheath far exceeds that of any peripheral cannula, enabling very high flow rates under pressure.
- Triple-lumen central venous catheter (CVC): A common misconception is that CVCs are equivalent to large-bore peripheral IVs for volume resuscitation. They are not. Each lumen of a standard triple-lumen CVC is typically 16G to 18G equivalent, and the length of central catheters increases resistance compared to short peripheral cannulas of the same gauge. CVCs are appropriate for medication delivery and monitoring; they are not the first choice for rapid volume resuscitation. An introducer sheath is preferred for that purpose.
How Does Bore Size Apply to Pediatric Patients?
Pediatric bore size selection follows the same principles but is constrained by the smaller caliber of pediatric veins. What constitutes large bore in a neonate or infant is very different from adult definitions.
For pediatric resuscitation, the PALS (Pediatric Advanced Life Support) guidelines recommend IO access early, within the first 60 seconds, if peripheral access cannot be established rapidly in a critically ill child. Attempts to place large-gauge peripheral IVs in a collapsed pediatric patient frequently fail and consume precious time.
In older children and adolescents, adult definitions apply more closely. A 10-year-old with adequate venous anatomy can often accommodate an 18G to 20G for emergency access. An infant requires 22G to 24G in the best available vein. A neonate requires 24G to 26G in dorsal hand, foot, or scalp veins.
Fluid resuscitation volumes in pediatrics are weight-based. The initial bolus for septic shock or dehydration is typically 10 to 20 mL/kg. At these volumes, the flow constraints of smaller gauges are less limiting than in adults requiring liter-scale resuscitation, but in pediatric trauma with significant hemorrhage, IO access remains the most reliable route for rapid large-volume delivery when peripheral access is not immediately available.
References
- https://pubmed.ncbi.nlm.nih.gov/7547060/
- https://pubmed.ncbi.nlm.nih.gov/2061178/
- https://pubmed.ncbi.nlm.nih.gov/29333494/
- https://www.mdpi.com/2227-9032/12/23/2445
- https://pmc.ncbi.nlm.nih.gov/articles/PMC4374744/
- https://professionaleducation.blood.ca/en/transfusion/clinical-guide/blood-administration
- https://www.sccm.org/clinical-resources/guidelines/guidelines/surviving-sepsis-guidelines-2021
- https://cpr.heart.org/en/resuscitation-science/cpr-and-ecc-guidelines/pediatric-advanced-life-support
- https://edge.sitecorecloud.io/americancoldf5f-acrorgf92a-productioncb02-3650/media/ACR/Files/Clinical/Contrast-Manual/ACR-Manual-on-Contrast-Media.pdf

