



What is an Anesthesia Circuit? Definition, Types, and Uses
Anesthesia Circuits
Ah, breathing: the gift our bodies give that keeps on giving. It is the act that keeps us going and an act that can be classified as both voluntary and involuntary, but sometimes, bodies need outside help from breathing systems, or anesthesia circuits. As a direct pathway to the body, breathing and the contents of what the body breathes directly affects the state of the rest of the system, physically and sometimes mentally too. Tinkering with the creation of a breathing system dates back to the 1900’s, when, in 1907, Barth developed a breathing system using just a valve and a nitrous oxide cylinder, a reservoir bag and Clover’s inhaler. Adjustment in the positioning of the lever in the valve revealed a range of ability to breathe, including complete rebreathing to breathing from the atmosphere. Magill’s circuit, a simple anaesthetic delivery system, was later made possible with the teamwork of a soft rubber single lumen tube, Boyle’s machine and endotracheal intubation.

The integration of cyclopropane in 1929 and cuffed endotracheal tube in 1931 lead to the “To and Fro” canister for closed system anesthesia with cyclopropane. As education in the field and more medical resources picked up, 1936 brought the circle system, followed a year later by Ayre’s T-piece, and the EMO inhaler four years later, followed by Minnitt’s ‘gas and air’ machine in 1949.
What is an anesthesia circuit?
An anesthesia circuit creates an artificial atmosphere, bringing anesthetic gases and oxygen from the home of an anesthetic gas machine to the patient. In the process, carbon dioxide and surrounding room air are removed, while temperature and humidity are preserved and kept regulated.
What is required?
According to Understanding Anesthetic Equipment & Procedures: A Practical Approach by Dwarkadas K Baheti and Vandana Laheri, the absolute basics of a breathing system must include the delivery of gasses from machine to the alveoli in the shortest time possible while maintaining concentration, the elimination of carbon dioxide, have minimal apparatus dead space and the implementation of low resistance. Resistance can be measured by the length times viscosity over radius to the fourth power. Endotracheal tubes, typically inserted through the mouth or nose, are most often the source of more resistance, further playing into the breathing in the anesthesia circuit. To minimize resistance, replace angle connectors with straight connectors, and utilize tubes and tube connectors with larger lumens.
What is desired?
Although not necessarily required, an anesthesia circuit ideally includes an economy of fresh gas, conservation of heat, and the appropriate amount of humidification of inspired gas. It should be light weight, convenient, and efficient. These factors are determined by carbon dioxide elimination and fresh gas utilization.
What is rebreathing?
As you may have guessed, rebreathing is the inhalation of previously exhaled gases. Fresh gas flow, mechanical dead space, and the anesthesia circuit’s design are all factors that determine the amount of rebreathing that is conducted.
Depending on the reservoir bag, rebreathing of exhaled gases, chemical neutralization of exhaled carbon dioxide and unidirectional valves, anesthesia breathing circuits may be classified as either open, semiclosed or closed.
In an open system, patients inhale gas from the anesthesia gas machine and exhaled gases are released into the atmosphere. A semiopen system allows for exhaled gases to flow from the system and back to the apparatus. Carbon dioxide is not absorbed and rebreathing is dependant upon the amount of fresh gas flow. According to Mary Karlet of Nurse Anesthesia Secrets, “if the amount of fresh gas flow supplied per minute is equal to or greater than the patient’s minute volume, no rebreathing occurs as long as exhalation is not impeded. A reservoir bag and unidirectional valves may be present.” In a semiclosed system, the exhaled gases partially redistribute into the atmosphere, and partially mix with fresh gases. In this case, a system to take in carbon dioxide, unidirectional valves, and a reservoir bag are utilized. In a closed system, complete rebreathing of gas takes place. In this instance, a system to absorb carbon dioxide, unidirectional valves, and a reservoir bag are included.
Mapleson F System
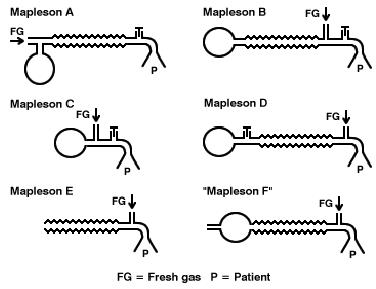
Mapleson F, the most common of the Mapleson systems, is also referred to as the Jackson-Rees System, as the original system was modified by Jackson Rees in the 1950’s with the addition of a common fresh gas inlet, corrugated tubing, an adjustable pressure limiting valve, and a reservoir bag. Commonly used to treat pediatric patients, it has minimal dead space and offers minimal resistance. It is an inexpensive, light and simple instrument, as it has no moving parts besides the overflow valve. Disadvantages include a need for fresh gas inflow to prevent rebreathing, potential for barotrauma and a lack of humidification.
Bain Circuit
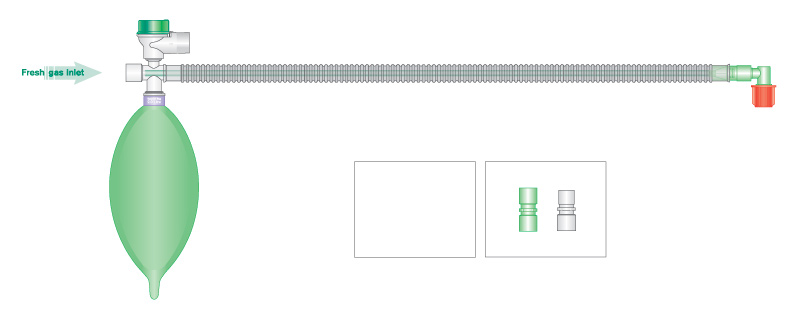
Also referred to as the Coaxial Mapleson D System, as the product came from evolution of the Mapleson systems. In the Bain System, the overflow valve is situated on the reservoir bag closest to the body, and fresh gas flows through a narrow inner tube, as part of an outer corrugated expiratory tube. One advantage is that with the fresh gas flowing in a separate tube that passes through the corrugated tubing, warming of the fresh gas inflow occurs. Moisture is also conserved due to partial rebreathing. There is ease of scavenging, and there is room to easily attach a ventilator.
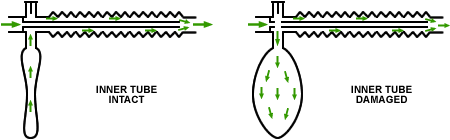
Some disadvantages are that monitoring the inner tube is difficult, although in most cases, the outer expiratory tube is clear, allowing inspection of the inner tube. Unrecognised detachment of the inner tube is possible, which would lead to carbon dioxide rebreathing.
Circle systems
According to openanesthesia.org, the circle system is the most popular system used in the US. Circle systems include a carbon dioxide absorber as a part of the system. Other necessary components include fresh gas entry, two unidirectional valves, inspiratory tubing and expiratory tubing that interconnect, a Y-piece that connects to the patient, a reservoir bag and a relief valve.
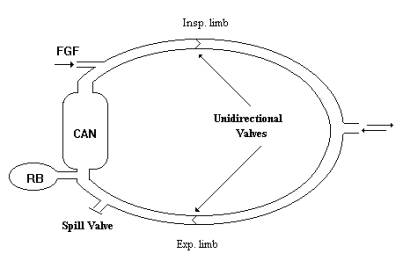
In circle systems, fresh gas inlet falls in between the reservoir bag and the inspiratory unidirectional valve. Fresh gas then flows through the inspiratory unidirectional valve to the breather. Backpressure allows this valve to close during exhalation and fresh gas continues to flow in a backwards motion to the reservoir bag. Airway moisture and heat are conserved due to the circular design, while pollution and waste of anesthetic gases are decreased. Some disadvantages include resistance to breathing, bulkiness, and potential for complexity. This system may be classified as semiopen, semiclosed, or closed, based on the fresh gas inflow.
Getting carbon dioxide out
There are two ways of releasing carbon dioxide from the anesthesia breathing system. The first is by a process called venting, where the exhaled gases are released into the atmosphere, by ways of open and semiopen systems. The other way is through chemical neutralization, done with semiclosed and closed systems. This process is done by passing exhaled gases through absorbent materials which may include soda lime or barium hydroxide lime.
References:
“Anesthetic Breathing Systems.” Understanding Anesthetic Equipment & Procedures: A Practical Approach. Ed. Dwarkadas K. Baheti and Vandana Laheri. New Delhi: Health Sciences, 2015. 114-22. Print.
Karlet, Mary. Nurse Anesthesia Secrets. St. Louis: Elsevier Mosby, 2005. Print.
“OpenAnesthesia.” OpenAnesthesia. N.p., n.d. Web. 15 Jan. 2016. <https://www.openanesthesia.org/anesthesia_delivery_systems_anesthesia_text/>.

